Thanks to vaccination, the incidence of FeLV has decreased significantly in the European feline population, and the same is true for the role of FeLV in the development of neoplasms.
The consequences of exposure to FeLV depend on the outcome of the battle between the virus and the cat’s immune system. On the viral side, the type of virus (A, B, or C for the most common), whether mutated or not, and the viral load come into play. On the animal side, vaccination status, immune status, and age at the time of infection are the main determining factors.
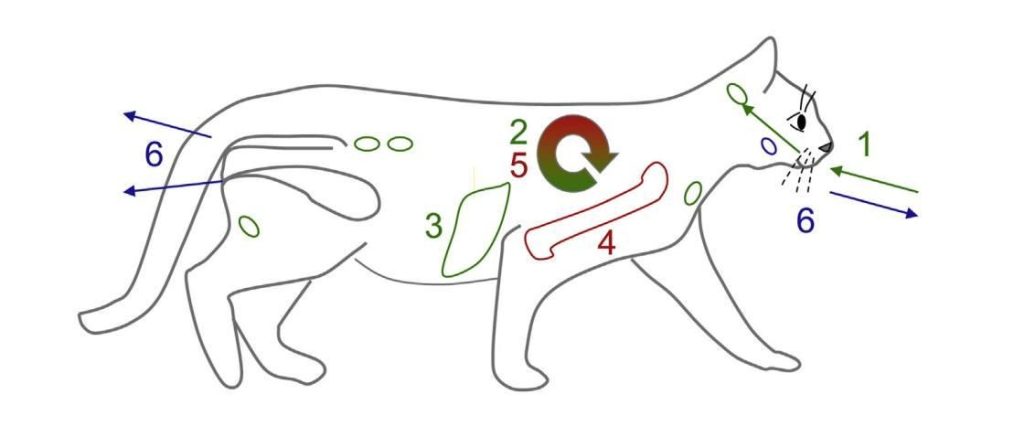
Four forms of FeLV
- Progressive infection: most likely to be associated with clinical signs, where the cat is shedding the virus and is therefore contagious to other cats.
- The latent infection: may remain asymptomatic for many years, or even the animal’s entire life. Reactivation is, however, possible, particularly in the event of a drop in immunity.
- Abortive infection: results in the eradication of the virus (approximately 10% of cases). The only sign of infection is the presence of circulating antibodies.
- Focal or atypical infection: rare, where only certain tissues are infected.
Generally speaking, the course of the infection is determined during the first 12 weeks.
Persistent viremia at 12 weeks (detection of p27 by ELISA + IFA) is the criterion for identifying a progressive infection. The cat is contagious. The virus is shed primarily through saliva and, to a lesser extent, through other excreta (urine, feces) or during pregnancy. The virus is fragile in the environment, so infections occur almost exclusively through direct contact. Thus, provided hygiene is maintained, infection between cats in separate cages during hospitalization is highly unlikely.
In cases of resolving infection, viremia may be transient or undetectable. ELISA or IFA (immunofluorescent antibody assay) for p27 are typically negative; however, circulating antibodies may be detected. The virus is integrated into the DNA of the cat’s bone marrow cells but does not replicate. The cat is not contagious but can transmit FeLV via a blood transfusion. Regressive infection is very rarely implicated in the development of neoplastic processes. It may, however, sometimes be associated with myelosuppression, most often erythroid (in 5.4% of cases according to one study). The diagnosis of a latent FeLV infection is based on the absence of p27 in the blood (ELISA and IFA), the presence of circulating antibodies (serology), and a positive PCR result on bone marrow.
Thus, a single positive FeLV test at the clinic (ELISA) is not necessarily detrimental to the animal’s life expectancy and quality of life. The p27 ELISA detects the presence of free virus in the blood, while the IFA detects the presence of the antigen in leukocytes: it is therefore more specific. False negatives are also possible during the first 2–3 weeks, as the virus is not yet circulating in the blood.
In a substantial number of cases, the disease may be asymptomatic or even eradicated. A second test at 12 weeks, preferably by IFA, helps determine whether the animal has a progressive form of the disease, which is most likely to result in clinical signs.
Source: What’s New in Feline Leukemia Virus Infection. Hartmann K, Hofmann-Lehmann R. Vet Clin North Am Small Anim Pract. 2020 Sep;50(5):1013-1036.